
Although Stars is not going anywhere, the combination of SY 2029 regulatory changes and the lawsuit mean more challenging times for Medicare Advantage plans.
NOTE: This blog is published in collaboration with Lilac Software, Inc. For more information on Lilac’s Stars Analytics Platform, see the end of this blog.
In a stunning decision, a federal judge in Georgia ruled in favor of Clover Health in its lawsuit challenging its 2026 Star Ratings. What’s more the judge seemingly has thrown out 20 measures in the program. The judge ordered just Cover’s 2026 ratings, impacting 2027 payments, to be recalculated. But it is hard to see how this could not impact all contracts if the ruling is upheld. Indeed, the Clover decision makes the 2024 Tukey cases and impacts look minor.
I do not believe Stars is going anywhere. It is too important to value-based care overall. But the decision does throw more uncertainty into Stars and plan finances. We undoubtedly will see appeals as well as action by the Centers for Medicare and Medicaid Services (CMS) and perhaps Capitol Hill. Note that CMS asked for an immediate reconsideration of the federal district court decision. The court did so late Friday but refused to change the decision after looking at an untimely brief from the government.
Let’s dive deep into the case itself and why such a major decision occurred.
Chevron and Loper guided the decision-making
To understand at least part of the decision by the judge, you must have a basic understanding of the long-standing and now repealed Chevron precedent as well as the Loper decision that over-ruled Chevron. The Chevron case was decided by the Supreme Court in 1984 and guided public policy regulations for four decades. In the Chevron case, the Supreme Court dictated that if a law passed by Congress was ambiguous, judges had to defer to a federal agency’s reasonable interpretation of that law. Fast forward 40 years to Loper Bright Enterprises. The high court overruled itself by throwing out Chevron, saying that federal administrative agencies do not have the relatively unfettered right to interpret ambiguous laws. Congress must make them clearer, or the judiciary shall interpret them.
This has led to a number of lower-court decisions since the Loper ruling where regulations have been overruled for not being strictly consistent with laws. A literal reading of statutes is now occurring in many cases. This also has led to inconsistent rulings in various courts because judges interpret statutes differently. This sets up the prospect of conflicting decisions on the same core statutes and regulations out there, potentially clogging the appellate levels and Supreme Court.
The Clover suit
Clover filed suit challenging its 2024 Medicare Advantage (MA) Star Ratings. Clover’s ratings dropped considerably in Star Year (SY) 2026, with 93% of its members enrolled in plans with ratings below four. This would cost Clover $120 million in bonus revenue in the future.
Clover’s arguments were very different than many prior lawsuits. Clover did not go down the road of most plans and argue that the calculation of measures is somehow wrong or arbitrary. Instead, Clover went after the ability of CMS to include measures in the program.
Clover’s two-prong argument that the court agreed: CMS and its parent Department of Health and Human Servies (HHS) do not have the authority to collect data and score certain measures in the Star program and CMS did not adequately notice changes or follow the Administrative Procedure Act (APA) for other measures.
On the issue of authority to include measures, Clover argued that the data for these measures were not collected under 42 U.S.C. § 1395w-22(e) as part of quality improvement programs and they were inappropriately considered in Star Ratings in 2026 because they were based on types of data not collected as of November 1, 2003. Specifically, Clover seems to argue that the quality program is limited to HEDIS, HOS, or CAHPS measures. Further, Clover also argued that new measures included in these categories generally could not be added post 2003 (but see more later).
The judge sided with Clover here, adopting the argument that only those areas specifically called out in the statute can be included in quality measurement and that Congress reined in the more liberal discretion CMS and HHS had earlier for the program. The court also concluded that Clover was right in terms of adding new measures in these categories later (in part because HHS did not report to Congress as required if they planned on doing so), although it did deem the Falls and Care Coordination measures as in the scope of CMS’ authority to add in the areas of CAHPS and HOS.
Clover also argued that some measure changes or inclusion did not conform to the notice and comment procedures of the APA, including that some have been added arbitrarily and capriciously. The court again agreed with Clover, arguing that the Stars measures program triggers the notice and comment rulemaking. This would seem to indicate that in the future CMS must rely solely on formal rulemaking rather than using in part its additional processes tied to the Advance Notice and Final Announcement as well as the annual Star Ratings Technical Notes.
The impact
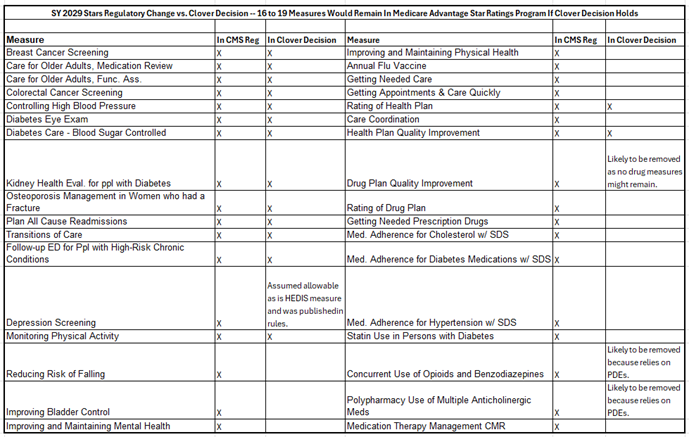
What measures are impacted and how does this jive with SY 2029 plans per the new 2027 MA and Part D rule that streamlines Star? Based on the two arguments, the 20 measures that cannot be included in Clover’s SY 2026 ratings and seemingly in the program as a whole are:
- C03 Annual Flu Vaccine
- C04 Improving or Maintaining Physical Health
- C05 Improving or Maintaining Mental Health
- C15 Reducing the Risk of Falling
- C16 Improving Bladder Control
- C22 Getting Needed Care
- C23 Getting Care Quickly
- C24 Customer Service
- C25 Rating of Health Care Quality
- C27 Care Coordination
- C32 Reviewing Appeals Decisions
- C33 Call Center – Foreign Language Interpreter and TTY Availability
- D01 Call Center – Foreign Language Interpreter and TTY Availability
- D05 Rating of Drug Plan
- D06 Getting Needed Prescription Drugs
- D08 Medication Adherence for Diabetes Medications
- D09 Medication Adherence for Hypertension (RAS Antagonists)
- D10 Medication Adherence for Cholesterol (Statins)
- D11 MTM Program Completion Rate for CMR
- D12 Statin Use in Persons with Diabetes (SUPD)
The 5 measures in bold are the overlap between what the court said needs to be eliminated and what was already sunset in regulation for SY 2029. The regulation sunset a total of 13 measures – three in SY 2028 and 10 in SY 2029. Depression Screening is added in SY 2029 under the final regulation and Medication Therapy Management Comprehensive Medication Review was set to return from Display. Thus, from SY 2027 to SY 2029, the number of measures was supposed to be reduced from 45 to 34 (with two Special Needs Plan measures included). But, if upheld, the Clover ruling would reduce the count from 34 to no more than 19 as 15 more measures would be eliminated (the non-overlap from the 20 above). The counts in each category would be:
- 13 HEDIS
- 1 CAHPS
- 1 HOS
- Possibly 2 Drug measures
- Possibly 2 Improvement measures
However, the two drug measures introduced in SY 2027 (COB and POLY-ACH) rely on what are known as PDE pharmacy claim submissions and that would seem barred under the ruling. If that is the case, the Part D Improvement measure would have no measures to gauge and thus would be removed. The Depression Screening in SY 2029 is a HEDIS measure that was included in a rule and that would seem consistent with the ruling. So, the number of remaining measures could actually be as low as 16.
What becomes immediately apparent is the following:
- Stars measurement becomes largely a HEDIS measurement program.
- We would have no or almost no measurement in Part D.
- The concept of gauging quality based on surveys is all but eliminated.
- The CAI and Reward Factor would need to be revamped.
- Improvement would apply to Part C only.
Who are winners and losers comparing SY 2029 status quo with the Clover decision?
I caution against drawing too many conclusions on winners and losers if the Clover decision wins out over the current SY 2029 plan from CMS. As I note above, there are many unknowns. But a quick review of performance on mostly HEDIS measures points directionally to the following:
- Some of the five big public plans get hurt.
- The innovative startups and growing players are helped.
- Blues have a bit of a mixed outcome.
- Integrated health systems with plans tend to win.
- And those with strong HEDIS results win.
So where does this leave Stars in the future?
I certainly do not begrudge Clover for challenging Star Ratings. And I do fundamentally agree that statutes and rulemaking should be followed. This is the only way to ensure the onerous hand of government does not squash transparency, due process, and a free market. I also do not think the judge’s ruling on the merits is wrong. It does appear that all elements of Stars as we know it today are not documented in the statutes. Further, it has been eminently frustrating for plans and interested parties to follow and cultivate Star road maps given the complexity of interim rules, final rules, advance notices, and final announcements. And as we saw with the 2024 Tukey and guard rail lawsuits, we do know that CMS does sometimes ignore statute and regulation.
But I do not think this ruling will hold or should hold for a variety of reasons. CMS will appeal the lawsuit and there is the possibility that the lower court decision will be stayed. That could allow the program to continue as is for some time. Given the huge policy and financial impacts, my bet is it will be put on hold at the appellate level.
My view is that both CMS and Congress would want to fix the issue. CMS has already moved to focus on a smaller set of measures for SY 2029 and beyond to better gauge quality improvement. And value-based care payments tied to quality have strong support within CMS and on Capitol Hill. There is reasonable alignment that quality should be measured for both Part C and Part D as well as via medical and clinical claims and member surveys. More to the point, more than half of all Medicare enrollees are in MA now. It is hard to fathom how a stump of a Stars program would be deemed adequate by lawmakers and policymakers alike.
And there is greasy politics. Large plans — likely impacted the most — will lobby for action to overturn the decision because it means billions of dollars to them. Then there are the midterms. MA benefits are already volatile and the meager 2027 rate increase could still mean additional benefit cutbacks and contraction. Lawmakers do not want to see even more impacts or voter distress due to concerns on Star ratings.
I would bet that Congress would act to affirm most or all of what CMS has planned for SY 2029 and maybe even broaden the statute again to provide greater flexibility to CMS on Stars, with some bounds. There also is the possibility that Congress could act to go a few steps farther on MA Stars reform, including making the program budget neutral (MA Stars is the only additive funding bonus I am aware of) and addressing how the Stars program measures quality (perhaps making it more local).
But the industry is in for a whirlwind just the same. Fixing the issue is no easy task and timing means that a number of years of Star ratings could be impacted if the decision is not stayed and ultimately overturned. CMS could repair some of this via regulation, but much of this would indeed take an act of Congress. That takes time.
While the judge only ordered that Clover’s Star Ratings be recalculated, that would be fundamentally unfair to many plans that would benefit from the decision. If CMS did not recalculate other plan ratings, lawsuits would undoubtedly be filed. So, no stay could lead to a hairy 2026 between adjusting Star Year 2026 ratings as well as announcing different SY 2027 ratings in October.
If CMS does what it did in SY 2024 (it gave contracts the better of the original calculation and the Tukey/guardrail court-mandated calculation), this could mean greater outlays for Medicare in payment year 2027. Quick math from examining CMS domain ratings (those who perform high on Part C Domains 1 and 2) suggests between 15% and 20% of 720 or so contracts (110 to 140 contracts) could see higher ratings under the Clover ruling recalculations, with a subset of those actually getting to 4 Star quality bonus revenue (most of them assuredly already had 3.5 ratings). Those getting added bonuses might be one-third to 40% of the 110 to 140. Take an average and do the math: that increases 4 Star and above contract by between 5% and 10%. Based on overall enrollment in MA and expected benchmarks in 2027, added bonuses could hit about $1B.
Given all of this turmoil and the cost to Medicare, CMS and Congress might decide to act sooner rather than later.
As an aside, Humana still has a lawsuit out there challenging its SY 2025 ratings. It hinges on the Call Center measures. It is possible that the Humana case could be positively influenced by this decision as the Clover judge threw out the Call Center measures (which are set to go away after this year). Indeed, a just-released filing in that case tells the Humana lawsuit court to look at the Clover decision.
What should plans do?
Plans obviously may want to be calculating Star ratings based on what is here now, what is scheduled to go in place in SY 2029, and what could be done due to the Clover decision. Such tracking is now a must moving forward to improve the right measures and maintain revenue across the various scenarios.
But if I were a plan, I would not overreact. We are seeing a seminal change in SY 2029 already. Focusing on the current measurement year with year-over-year quality improvement as well as plotting strategy for the known regulatory changes should be top of mind. My crystal ball says that drug measure evaluation will be back as will fulsome CAHPS and HOS surveys. The fundamentals of the SY 2029 reforms will stay.
At the same time, plans need to discuss a legal strategy. This is a threshold issue for plans and revenue. What recourse do you have based on your prior engagement with CMS on Stars data discrepancies and rating concerns? Will you file a suit (and on what legal basis) based on any of the possible scenarios that could result as the case winds and wends through the court system? How will you engage lawmakers and CMS?
Note: This blog was published in collaboration with Lilac Software. To learn more about Lilac Software’s Stars Analytics Platform and agentic AI solutions, visit https://lilacsoftware.com.
#stars #cms #medicareadvantage #partd #quality
— Marc S. Ryan



