
NOTE: This blog is co-published in collaboration with Lilac Software, now part of MediSolv. To learn more about Lilac’s Stars data analytics and agentic AI solutions, visit https://lilacsoftware.com
Star Rating changes will lead to major volatility and revenue loss for many MA plans
The Centers for Medicare and Medicaid Services (CMS) finalized the 2027 Medicare Advantage (MA) and Part D rule. While much of the rule did not have earth-shattering changes, it is safe to say that the major Star ratings reforms will have far-reaching impacts on MA plans for years to come.
Star changes
Let’s first inventory the Star changes. The proposed rule changes were all adopted with just one exception. CMS says these changes refocus the program on clinical care, outcomes, and patient experience where meaningful performance differences exist across contracts and reduce administrative burden by removing measures that provide little meaningful distinction between plans.
The changes break out this way:
- The cancellation of the Excellent Health Outcomes for All (EHO4all) reward while maintaining the Reward Factor was finalized. This was despite the effective retroactive removal of the EHO4all in Star Year (SY) 2027. While some plans had invested a lot in building health equity capabilities, CMS moved forward anyway. Most of the big plans and trade associations put up little fuss on the change so CMS felt empowered to make the retroactive change. While plans have litigated in the past, I don’t see a huge movement to do so here. This most hurts dual eligible penetrated plans and Special Needs Plans (SNP) that don’t benefit from the Reward Factor and were counting on the boost from EHO4all.
- All of the proposed measure terminations were adopted except the Diabetic Eye Exam measure was maintained. The 13 measure eliminations and the SY they are effective are:
- Call Center (2) in SY 2028
- Part C Appeals (2) in SY 2029
- Leave (2) in SY 2029
- Complaints (2) in SY 2029
- Special Needs Plan-Care Management in SY 2029
- Medicare Plan Finder in SY 2029
- Rating of Health Care Quality in SY 2029
- Customer Service in SY 2029
- Statin Therapy for CVD in SY 2028
- Depression Screening will also be added as of SY 2029.
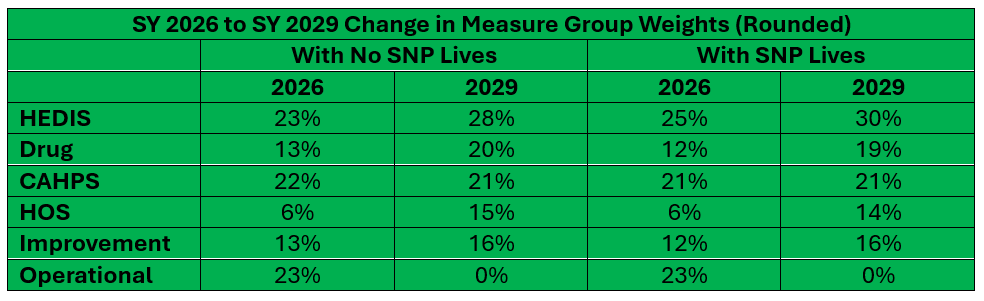
Group weighting changes
The retirement of the measures creates a huge change in the relative weights of measure groupings. In general, the impact of clinical measures (HEDIS and Drug) as well as survey measures (CAHPS and HOS) increases dramatically. Clinical measures will now be almost half of the rating, with survey measures over one-third.
The impact
In its draft rule notice, CMS indicated about one-quarter of all contracts would see a half Star decrease in their ratings when the changes are fully implemented. But what these statistics don’t tell you is that many other contracts could also see erosion in their Star rating, just not enough to cause a half Star rating reduction. For these other plans, they are then that much further away from increasing their Star rating. Overall, the operational measures were high performing compared with other measure groupings for many plans. Generally speaking, full SNP plans tend to get hurt the most. While some large plan contracts are impacted, larger organizations are less impacted than smaller and medium ones.
Several actuarial firms indicate that impacts are worse than CMS says. Based on the proposed rule, a Milliman white paper shows 30% of contracts could lose half a Star, with a few dropping a full Star. At least 42 contracts may fall below the 4.0 Star level. The number of contracts below 3.5 Stars also increases by 63. And showing the impact on other contracts, the national contract-weighted average for overall Star achievement could decrease by 0.15 Stars.
Wakely Consulting’s analysis dovetails with the impacts found by Milliman. It says the national enrollment-weighted market average for overall Star achievement will drop by 0.25 Stars. This will mean a loss of revenue of 1.4% for MA-Part D (MA-PD) plans and fewer 4 Star plus contracts. The lower Star ratings impact plans of all sizes — top 10, large, mid-size, and small.
Other analyses, inlcuding our own, see deep consequences as well. Some say that as many as 41% of contracts could lose half a Star and about 90% of contracts will see a decline in their overall contract rating. The number of contracts receiving a 4-Star or greater bonus will drop from about 40% in SY 2026 to 28% in SY 2029. Between $1.3B and $2.2 billion could be lost in quality bonus.
The quirky economics of all this is that the reversal of the EHO4all reward and maintaining the Reward Factor means better Star bonuses in the short term for some contracts, especially larger ones. But for those not getting a Reward Factor, the economics are bad from the start.
CMS also finalized a technical clarification from the CY 2026 MA and Part D proposed rule related to contract consolidations.
Enrollment, benefit, and clinical oversight changes
Here is an overview of the non-Star changes finalized. A few proposals were not accepted in the end as well.
Provider Network SEP: A special enrollment period (SEP) that would have allowed enrollees to switch plans when their provider leaves their MA network was not finalized. CMS said it will consider it for future rulemaking. Other existing SEP policies were codified.
SSBCI Eligibility: A requirement that plans publicly post their eligibility criteria for Special Supplemental Benefits for the Chronically Ill (SSBCI) was finalized. Eligibility requirements were also clarified.
SSBCI Cannabis Prohibition: Language was adopted to prohibit coverage of cannabis products that are illegal under federal or state law.
Supplemental Benefit Notification Repeal: The final rule removes the requirement for plans to issue mid-year notices regarding unused supplemental benefits.
Health Equity Provisions Repealed: The final rule removes requirements for (1) MA utilization management committees to include a health equity expert, (2) the duty to conduct publicly posted annual health equity analyses, and (3) for quality improvement programs to include activities specifically designed to reduce health disparities.
Account-Based Plan Relief: Language to exempt account-based plans (such as health reimbursement arrangements (HRAs), flexible spending accounts (FSAs), and health savings accounts (HSAs)) from creditable coverage disclosure requirements was adopted.
Marketing and related changes
Waiting Period Relief: The final rule eliminates the 48-hour waiting period between completing a Scope of Appointment (SOA) and holding a personal marketing appointment. The rule also eliminates the mandatory 12-hour waiting period between an educational event and a subsequent marketing event at the same location. Other marketing reforms were finalized to bring flexibility.
TPMO Reform: Key changes impacting Third-Party Marketing Organizations (TPMOs) and marketing were adopted, including updated language specifying the number of organizations and plans TPMOs represent, continuation of the TPMO disclaimer verbally during sales calls, and reduction of the required retention period for recordings from 10 years to 6 years.
Superlatives Allowed: The final rule removed the explicit prohibition on superlatives such as “best” or “most” in marketing materials, but marketing content cannot be misleading, confusing, or materially inaccurate.
Dollar Value Marketing: A proposed ban on marketing the dollar value of supplemental benefits was not finalized.
Debit Cards: CMS finalized guardrails related to the use of debit cards in supplemental benefits. Plans using debit cards to administer supplemental benefits must link cards to a real-time, point-of-sale verification mechanism and limit card use to the specific plan year.
Inflation Reduction Act codification
CMS finalized the codification of Part D changes under the Inflation Reduction Act (IRA), including:
- The elimination of the coverage gap.
- The reduction of the annual out-of-pocket threshold to $2,000.
- Removal of cost sharing in the catastrophic phase.
- Updates to True Out-of-Pocket (TrOOP) cost calculations.
- Clarification related to specialty-tier drugs, reinsurance payments, and subsidy structures.
- Implementing the Manufacturer Discount Program that replaced the Coverage Gap Discount Program.
Requests For Information (RFIs)
CMS sought public input on future modernizations in three areas. The agency received more than 42,000 comments on the proposed rule overall but said little else in the final rule in terms of the comments.
Risk Adjustment and Star Ratings Programs: CMS sought broad input on changes to reform and modernize the risk adjustment and quality bonus payment systems.
The risk adjustment request stemmed from the overpayment controversy at large plans and views that the system may discriminate against smaller, newer, and regional plans. CMS may want to migrate to an encounter-based rate-setting system.
Some within CMS and on Capitol Hill also want the Star program to be budget neutral and not additive in terms of funding. MA has the only quality bonus that comes from added dollars. CMS also wants to reduce the two-year time lag in ratings.
Oversight of Chronic Condition Special Needs Plans (C-SNPs) For Dually Eligible Individuals: C-SNPs have grown demonstrably over the past two years. Dual Eligible Special Needs Plans (D-SNPs) were meant to enroll dual eligibles, but more and more are going into the fast-growth C-SNPs. CMS may want to require state Medicaid contracting for C-SNP as well as Institutional Special Needs Plans (I-SNPs).
Well-Being: Coverage of well-being (including preventive care, mental health, and social connections) and nutrition policies. Additionally, CMS sought public input on approaches and opportunities to streamline regulations and reduce burdens on those participating in the Medicare program through a standalone RFI.
In addition, in the proposed rule, CMS also asked for input on modernizing marketing oversight and agent/broker regulations.
#cms #regulations #medicareadvantage #partd #pdp
To learn more about Lilac Software’s Stars data analytics and agentic AI solutions, visit https://lilacsoftware.com
— Marc S. Ryan



